Our journey started with a sunny day. We reached our destination at 8.25am. Before the session started, a few of us went to pharmacy to take a picture of soft gel, and a picture of Advanced Quality Rapid Anti-HIV (1&2) test kit. The officer who is in charge in the laboratory department showed us the kit. He asked one of us to be a volunteer for the Rapid HIV test as the test kit is sealed in a sterile plastic packet. Once it is opened, it must be used.

Nutritional supplement for pregnant/lactating women

Rapid Anti-HIV Kit Test

Intended Use:
Advanced Quality Rapid Anti-HIV (1&2) test is a colloidal gold enhanced, rapid immunochromatographic assay for the qualitative detection of antibodies to human. Immunodeficiency virus (HIV) in human whole blood, serum or plasma. This test is a screening test, and all positives must be confirmed using an alternate test such as western blot. The test is intended for healthcare professional use only.
Summary
1. The human immunodeficiency virus (HIV) is the causative agent of acquired immune deficiency syndrome (AIDS).
2. The general method of detecting infection with HIV is to observe the presence of antibodies to the virus by an EIA method followed by confirmation with Western Blot.
3. The Rapid Anti-HIV (1&2) Test is a simple, visual qualitative test that detects antibodies in human whole blood, serum or plasma. The test is based on immunochromatography and can give a result within 15 minutes.
Principle of the procedure
- The assay starts with a sample applied to the sample well and add provided sample diluent immediately.
- The HIV antigen -colloidal gold conjugate embedded in the sample pad reacts with the HIV antibody present in whole blood, serum or plasma sample forming conjugate/HIV antibody complex.
- As the mixture is allowed to migrate along the test strip, the conjugate/HIV antibody complex is captured by a second antibody immobilized on the membrane forming a colored test band in the test (T) region.
- A negative sample does not produce a test band due to the absence of colloidal gold conjugate/HIV antibody complex.
- The antigens used in the conjugate test are recombinant proteins that correspond to highly immunoreactive regions of HIV1 and HIV2.
- A colored control band in the control (C) region appears at the end of test procedure regardless of test result. This control band is the result of colloidal gold conjugate binding to the anti-HIV antibody immobilized on the membrane. The control band indicates that the colloidal gold conjugate is functional.
Reagents and Materials Supplied:
– Test cards individually foil pouched with a desiccant.
– Plastic dropper
– Sample Diluents
– Safety lancet
– Alcohol swab
– Package Insert
– Plastic Pipette to dispense sample

SPECIMEN COLLECTION
1. Clean the area to be lanced with an alcohol swab.
2. Squeeze the end of the fingertip and pierce with the safety lancet as instructions below.
Assay procedures
- Dispense 1 drop (10 µl) of whole blood, serum or plasma to the circular sample well of the test card using the plastic dropper provided according to the figure.
- Add two drops of Sample Diluent to the sample well immediately after the specimen is added.
- Interpret test results at 15 minutes.
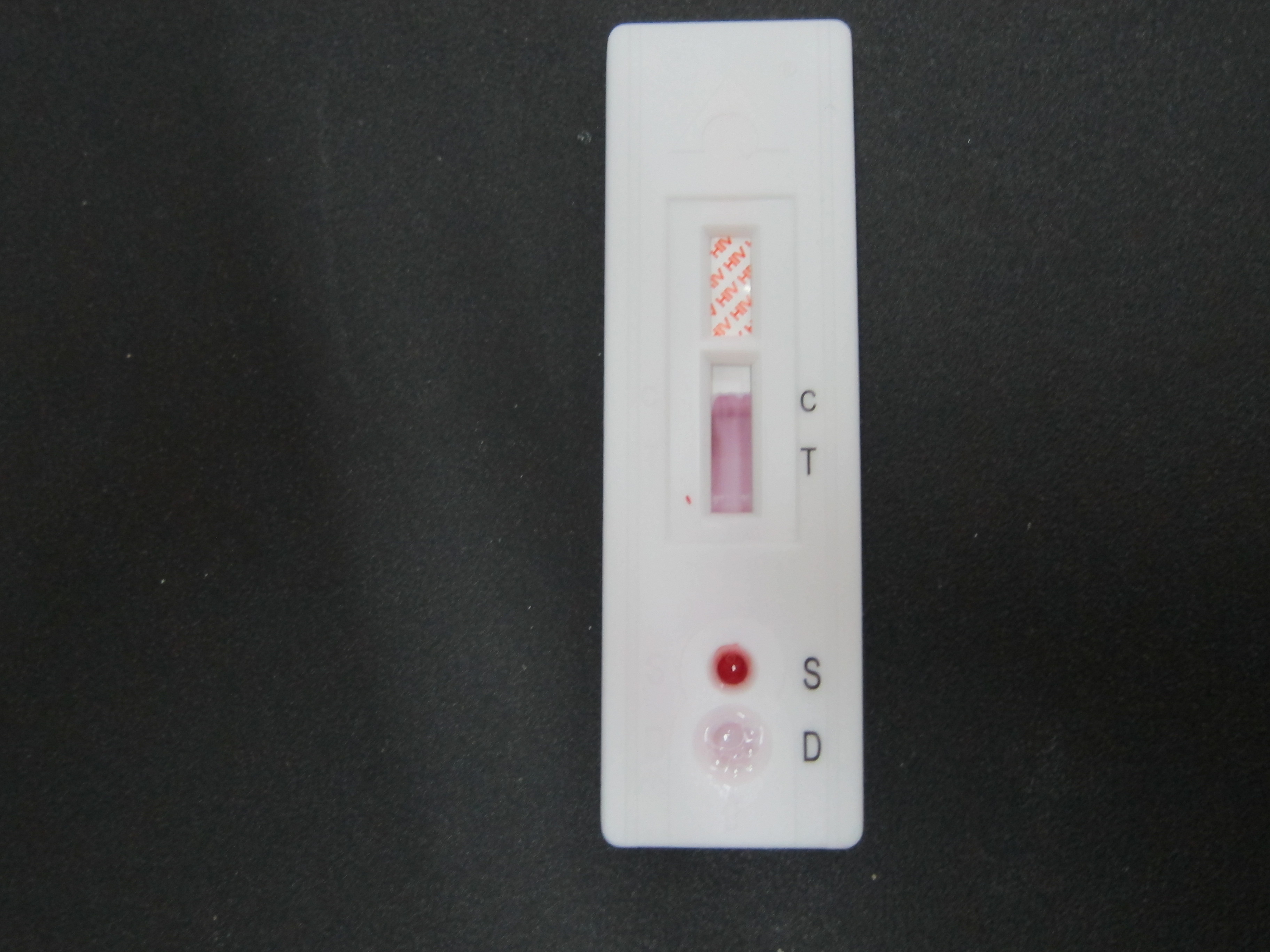
Reading the test results:
- Positive: Both purplish red test band (T) and purplish red control band(C) appear on the membrane. The lower the antibody concentration, the weaker the test band.
- Negative: Only the purplish red control band (C) appears on the membrane. The absence of a test band (T) indicates a negative result.
- Invalid: There should always be a purplish red control band in the control region regardless of test result. If control band (C) is not seen, the test is considered invalid. Repeat the test using a new test device.
Note: It is normal to have a slightly lightened control band with very strong positive samples as long as it is distinctly visible.
Limitations
1. Only samples that are clear and with good fluidity can be used in this test.
2. Fresh samples are best but frozen samples can be used. If a sample has been frozen, it should be allowed to thaw in a vertical position. Do not agitate the sample. Insert a pipette just below the surface of the sample to collect the specimen.
After that, we went back to the Meeting Room. The speaker of the day was PPKP Mr. Muhamad Fahmi. He briefly talked about Non-Communicable Disease (NCD) unit. He explained about the jobs and responsibilities of the unit. He is also in charge in the enforcement of Tobacco Regulation.

Cigarettes that were compound
Next, he introduced us about Klinik Berhenti Merokok (KBM), Quit Smoking Clinic.
Quit smoking clinics are available in hospitals and health clinics to help smokers to quit smoking with proven techniques that is behavior modification therapy and nicotine replacement therapy. There are 2 Quit Smoking Clinics in Sik. One in KK Jeniang, another one is in KK Gulau.
Mr. Fahmi is also in charge in monitoring nurseries, kindergarten, PASTI, and private nurseries (whether the premises are safe to be used, monitors the cleanliness of the premises, any cases of Hand, Foot, and Mouth disease in these premises.)
Besides, he also cooperates with Pegawai Zat Makanan in BMI Screening Weight Management.
After the talk, we went to KBM in KK Jeniang. This KBM started in 2009 in KK Jeniang.
Procedure:
Registration of the smokers
Evaluate any risk factors (DM, HT, etc)
Blood is taken for lipid profile (counseling is given by Medical Assistant)
Medical Officer (counseling and decides which therapy to be given to the smokers)
For beginners: Behavior modification therapy
For heavy smokers: Nicotine Replacement therapy
Mr. Azrullah explained about Champix (tablets used in Nicotine Replacement Therapy). Each tablet is 1mg. This therapy is indicated for heavy smokers (30 sticks/day). Those who are not heavy smokers, they will undergo behavior modification therapy.

Champix
The following is the dosage of the tablet to be taken:
1st 3 days – 0.5mg OD
4th-6th days – 0.5mg BD
7th day onwards – 1mg OD
Duration of each cycle is 2 weeks. After 2 weeks, Mr. Azrullah will assess the smoker. If the smoker is able to quit smoking after taking Champix for 2 weeks, this indicates he succeed in quit smoking program. However, if he is not able to quit smoking after taking Champix for 2 weeks, this therapy will continue for 6 months. Maximum duration of the therapy is 6 months. If he is still unable to quit smoking after 6 months of therapy, the result is considered as failure.
Mr. Fahmi explained to us how to define a person who quit smoking. It is defined as a person who does not smoke for 6 months from the day he starts the treatment.
That’s all for today.





































{kind=link}